
designer drugs
At the moment there are several dozen types of drugs – from widely known to unfamiliar exotic and just very rare. Some time ago, little was known about drugs. Today, psychotropic and narcotic substances themselves, or references to them in the mass media, have become common to many. We give the main ones.

Hallucinogens (substances that can cause not only euphoria, but also hallucinations)
lsd, cannabinoids, ketamine, mescaline, psilocybin, phencyclidine, dimethyltryptamine.
Opioids (substances affecting the mu-opioid receptors and, by their clinical effect, narcotic analgesics that cause euphoria in combination with sedation)
heroin, desomorphine, codeine, methadone, morphine, opium, fentanyl, tramadol.
Psychostimulants (substances that also cause euphoria, but in combination with stimulation of the nervous system)
amphetamine, captagon, cation, cocaine, MDA, methamphetamine, methylphenidate, methcathinone, nicotine, extasy, ephedrine.
Depressants (substances that inhibit the central nervous system or suppress and reduce certain aspects of its activity)
barbiturates, benzodiazepines, butyrate.
Antidepressants (substances that block the breakdown or reverse neuronal seizure of monoamines (serotonin, norepinephrine, dopamine, phenylethylamine, etc.) under the action of monoamine oxidase
coaxil
Inhalants (Volatile narcotic active substances in the form of gas or volatile liquids that are inhaled in order to achieve euphoria and a hallucinogenic effect. This type of addiction is called substance abuse)
nitrous oxide, aromatic and aliphatic hydrocarbons.

At present, it is unlikely that anyone will take up the compilation of a complete list of existing dispensary drugs, the number of which, apparently, has already exceeded a thousand and continues to grow.
The emergence of all new drug drugs is primarily possible due to the progress in chemical synthesis, when a new substance can be synthesized from available chemicals with appropriate chemical reactions, having predetermined properties, including psychoactive ones. The development and improvement of chemical synthesis technology has led to the fact that since the middle of the last century, the production of disaner drug began to move from opium, cocaine or hemp plantations to chemical laboratories. The production and consumption of disaner narcotics created (synthesized) in chemical laboratories is becoming increasingly widespread every year. Thus, synthetic stimulants (amphetamine, methamphetamine and ecstasy) ranked second in the world (after cannabis) in terms of the scale of their consumption, surpassing the total consumption of heroin and cocaine (UNODC, 201 lb). The simplicity and cheapness of the production of many synthetic disanergy drugs, the absence of the need for expensive chemical equipment, the availability of the initial components, the slowness of the legal system — all this leads to the fact that new synthetic disanergic drugs regularly appear that do not fall under existing control measures your legal status.
The creation of new drug-related drugs goes in two main directions. First, using chemical synthesis, it is possible to obtain substances that, sometimes unexpectedly for the creators themselves, become known as dispensary drugs, although they were originally created for other purposes (what happened, for example, with amphetamine, methaqualone, MDMA, etc.). The second direction, which also leads to the emergence of new disanerny drugs – this is the so-called. Design Disaner drug. In this case, we are talking not so much about creating previously unknown disanernykh drugs, as about a certain chemical “alteration” of existing ones, in which they retain (or even strengthen) their former properties, but have a chemical structure different from the “original”.

Sometimes designers of designer drugs get a substance whose properties are far from the expected ones. One of the most famous stories in this area occurred at the end of the 70s. in USA. In 1976, a 23-year-old chemical student Barry Kidston (Barry Kidston) decided to independently synthesize 1-methyl-4-phenyl-4-propionoxypiperidine (l-methyl-4-phertyl-4-propionoxypiperidine– MPPP), which is a derivative of meperidine (meperidine). MRRR has been known since the 40s. as a synthetic opioid analgesic, but it is not used in clinical practice.
There is an increased interest in designer designer drugs from clandestine manufacturers, for several reasons. First of all, as mentioned above, due to the changed chemical structure, designer disanergic drugs, after their creation, do not fall under the existing prohibitions and restrictions concerning their prototypes and therefore can be produced and distributed without hindrance during a certain period of time. This circumstance allows manufacturers of such dizanerskih drugs to launch a broad and for the time being quite legal advertising campaign to promote a new product to the market, under some catchy names. Such disinhering drugs can be advertised as various dietary supplements, weight loss products, incense kits, body care products, etc. Another reason is that experts often do not have methods and means of identifying such drugs. Existing methods are often insensitive to new disanernyh drugs, which is an additional factor that increases the period of their uncontrolled use.

synthetic cannabinoids
synthetic cannabinoids cathinone narcotic chromatography
This concept is currently collective in nature and is used to denote a wide range of products that represent aromatic herbal mixtures of different composition that are formally intended for various incense, but not for smoking, as warned by the corresponding inscriptions on a number of packages: “not for human consumption “(” Not for human consumption “). Despite this warning, which is of a formal nature, smoking is the main way of using synthetic cannabinoids.
synthetic cannabinoids began to gain fame in the United States and European countries since 2006, although the first samples of such mixtures appeared, most likely, in 2004 (EMCDDA, 2009; Vardakou et al., 2010). The main distribution channels of cannabinoids synthetic are online stores, various specialized retail outlets and individual distributors. The product is advertised as a safe herbal mixture for incense (or for smoking). There are no age restrictions on the purchase of this product in most cases, which contributes to the growing popularity of synthetic cannabinoids among young people (Vardakou et al., 2010).
As information about the effects of smoking on cannabinoids synthetic began to accumulate, experts began to express doubts about the ingredients on the package. Self-reports of smokers of cannabinoids synthetic left no doubt that it produces a psychoactive effect. Since the composition of the herbal mixture indicated on the packaging is not able to cause the effects that were observed among lovers of synthetic cannabinoids, in various countries since 2008, analyzes have been carried out on what is actually contained in a sachet of cannabinoids synthetic or other similar products (Auwarter et al., 2009).
The results of the tests confirmed the concerns of specialists. Synthetic cannabinoids, which are agonists of the so-called CNS present in the CNS, were found in the “safe herbal mixtures”. cannabinoid receptors. After the release of tetrahydrocannabinol (THC) in the 1960s, a large number of synthetic cannabinoids were obtained. Synthetic cannabinoids were found in synthetic cannabinoids and other similar herbal mixtures, in most cases belonging to four main groups (Auwarter et al., 2009; EMCDDA, 2009; Uchiyama et al., 2010; Vardakou et al., 2010).
The first of them includes those that are as close as possible in their chemical structure to THC and, in fact, are its synthetic analogues.
The most popular representatives of the first group are such synthetic cannabinoids as HU-210 nabilone, dronabinol (dronabinol), etc.
They find definite medical applications, for example, in the treatment of nausea after chemotherapy.
The second group combines synthetic cannabinoids derived from synthesized in the 70s. the pharmaceutical company Pfizer cyclohexylphenol (cyclohexylphenol – CP), for example, CP-47.497, CP-59.540, etc.
The third group includes synthetic cannabinoids from among those synthesized in the 90s. A group of researchers from Clemson University (South Carolina, USA) headed by Professor John William Huffman. They are designated by the first letters of his name and surname: JWH-018, JWH-015, etc. In herbal mixtures in recent years, synthetic cannabinoids belonging to this group, first of all, JWH-122 and JWH-210, are becoming increasingly common. This is of particular concern to specialists, since JWH-122 and JWH-210 have strong psychoactive potential and their use as a part of synthetic cannabinoids leads to serious and hardly predictable consequences.
The fourth group includes various chemical compounds (for example, based on derivatives of oleic acid), whose status as a synthetic cannabinoids is uncertain.
After the discovery of the synthetic cannabinoids in the synthetic cannabinoids, many countries began to introduce bans and restrictions on the distribution and sale of herbal mixtures. Since synthetic cannabinoids are not subject to the international conventions on narcotic drugs and psychotropic substances, each country independently determines their legal (legal) status (EMCDDA, 2009).
Studies have shown that most synthetic cannabinoids found in synthetic cannabinoids have a stronger effect on the body than cannabis-containing THC. This is due to the fact that natural THC and synthetic cannabinoids have a different effect on the so-called. cannabinoid receptors present in the brain.
“Bath salt”
As in the previous case, we are talking about the collective name of a wide range of products, produced under various names and in most cases formally related to household chemicals (from bath salts and insect repellent to jewelry cleaning products or wiping mobile phone screens ). The variety of names hides disaner drugs, which are synthetic analogues of psychoactive alkaloids contained in kata leaves (Cathaedulis, or cat edible), an evergreen shrub that is widespread in several countries in East Africa and the Arabian Peninsula (Somalia, Kenya, Ethiopia, Djibouti, Yemen, Saudi Arabia and others.).
Kata leaves contain a number of psychoactive alkaloids, primarily cathinone (cathinone) and cathine (cathine). The mechanisms of their action are not much different from the actions of cocaine and amphetamine. Cathinone and cathine prevent the reuptake of norepinephrine and dopamine in the synaptic cleft, which leads to an increase in their concentration and, consequently, to a stimulating and euphoric effect. Compared with cocaine and amphetamine, the effect of cathinone and cathine is more “soft”, not so strong and not so intense.
The main active principle of kata is cathinone. Katin has a very weak psychoactive effect and manufacturers of synthetic drugs have no special interest in relation to him. As for cathinone, there are currently about 30 of its synthetic analogues, which have a pronounced psychoactive potential (ACMD, 2010; EMCDDA, 2012). Some synthetic cathinones (bupropion, pyrovalerone) have certain medical uses, for example, in treating depression, stopping smoking or treating chronic fatigue, but due to the threat of their abuse their medical use is extremely limited (Prosser & Nelson, 2012).
If you go back to the “bath salt”, then this product consists of a single species or a mixture of several synthetic cathinones. Most often we are talking about such a synthetic cathinone, as 3,4-methylenedioxypropyl (3,4-methylenedioxypyrovalerone – MDPV), but other synthetic cathinones can be included in the bath salts: mephedrone (mephedrone), butylone (butylone) , piroverone (pyrovalerone), methedrone (methedrone), methylone (methylone), methcathinone (methcathinone), etc.
Synthetic cathinones are available in various forms. If it is a “bath salt” or “plant food”, it is white or brown powder. In other cases, it may be capsules or tablets. The declared purity of the product may exceed 95%, but the consumer has no real opportunity to check how this corresponds to reality. The ways of using synthetic cathinones (independently under the “cover” of what brand they are sold) are not much different from the ways of using other dispensary drugs. The powder can be inhaled through the nose in a manner that is slightly different from cocaine use. Tablets and capsules are taken orally. Sometimes small pellets are rolled out of powder and tissue paper, which are then swallowed. Less commonly used are intravenous or intramuscular injections and rectal or vaginal use. Smoking is not very popular because synthetic cathinones are destroyed when heated (ACMD, 2010; EMCDDA, 2012).
The size of the dose taken varies in a wide range of its values (from a few milligrams to 1 g and above), depending on the method of use and the quality of the substance used. The average dose size is from 5 to 20 mg (Ross et al., 2011) In case of powder inhalation, its action begins after 5–20 minutes, then, after 15–30 minutes, the peak of the effects produced is reached, after which they enter the plateau phase lasting up to two hours. After the plateau, there is a weakening of the action of disaner narcotics, which takes from 30 to 60 minutes. The total duration of the effects produced ranges from 2 to 3.5 hours. When taken orally, the effect of the dose taken begins after 15-30 minutes and can last up to 7 hours (Erowid, 2011).
The physiological and psychological (behavioral) effects caused by the use of synthetic cathinones are not well understood. Information about them is mainly based on subjective consumer self-reports and medical reports. Typical effects include tachycardia, dangerous increases in blood pressure, hyperthermia, insomnia, loss of appetite, gastrointestinal disorders, bruxism (gnashing of teeth), nausea, tinnitus, dizziness, difficulty breathing, headache, pupillary dilation. In the case of injections, skin abscesses, ulcers are typical, and necrotic fasciitis can develop (a progressive infection process leading to necrosis of the subcutaneous tissue, including fascia and adipose tissue), often requiring radical surgical intervention. As the dose increases, the risk of renal, cardiac and respiratory failure, seizures, and death increases (Ross et al., 2011).
Psychological effects include general emotional and emotional growth, improved mood and euphoria, a feeling of energy flow, clarity of thought, increased sociability and empathy, sexual arousal, hyperactivity. As the dose increases, or in the case of repeated doses, anxiety begins to grow, and anxiety, accompanied by panic attacks, increases significantly. The appearance of psychosis, paranoid delusions, confusion, auditory and visual hallucinations, and crawling sensations are typical. Aggressive behavior is possible, including self-harming, attempted suicide, and attempted murder (James et al., 2011; Ross et al., 2011; Prosser & Nelson, 2012).
 Cannabinoids
Cannabinoids  Codeine, Dihydrocodeine
Codeine, Dihydrocodeine  Barbiturates
Barbiturates 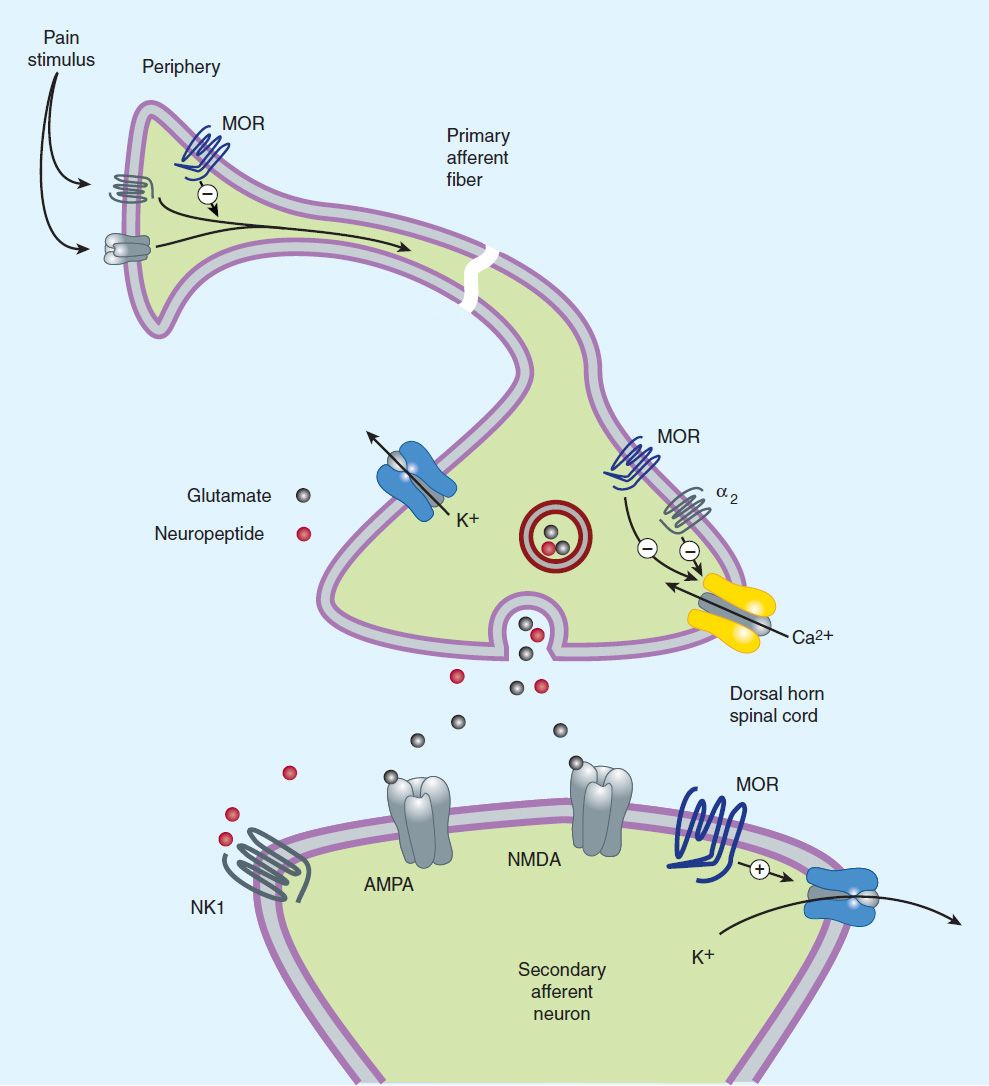 Opium antagonists
Opium antagonists  Fentanyl
Fentanyl  2C-B
2C-B  MGM-15
MGM-15  PiPTapentadol
PiPTapentadol  Methoxptamine (MXP)
Methoxptamine (MXP)  Nortilidine
Nortilidine
Just my thoughts about Spice, the first one of a kind branded cannabinoid blend.
One of the first very popular brands.
Was so called Spice.
There were several products from the same manufacturer, the most powerful and famous, was called
Spice Gold.
There were 1g and 3g bags available,
There was also silver, arctic, diamond – those were all crappy, compared to the OG”Spice Gold”
With very catchi designs.
They sold many million bags and were the very first that hit the market,
especially here in Germany I saw it as one of the first to be a one of a kind product and starteted a Spiceshop..
The product was sold nearly everywhere,
in Headshops and every “alternative” shop,
Even where afroshops, herbal and shishashops, also tobaccoahops.. It was sold everywhere till the first ban.. It was the spice “Goldrush”..
Then, Nearly till now it’s sold or was sold under the table, to customers that know where to go, what to ask or just logically longterm supplied buyersand their friends..
Best regards
doNzen